A couple of weeks ago I announced the imminent death of colloid. Now it’s back with another “Safe” trial (known as CHEST) from our colleagues in Australia and New Zealand (here). The study enrolled a colossal number of patients (7000) to either isotonic saline (IS) or Voluven (R). This is a 130/0.4 tetrastarch in isotonic saline. I now understand the kerfuffle over the 6s trial (of tetraspan) that mislabeled 130.42 in balanced salt as 130/0.4 (read here). The paper should be subtitled: “ours – the starch that doesn’t kill!” Perhaps…
The authors randomly assigned 7000 patients who had been admitted to an intensive care unit (ICU) in a 1:1 ratio to receive either 6% HES with a molecular weight of 130 kD and a molar substitution ratio of 0.4 (130/0.4, Voluven) in 0.9% sodium chloride or 0.9% sodium chloride (saline) for all fluid resuscitation until ICU discharge, death, or 90 days after randomization. The patients were permitted 50ml/kg HES per day and then were given saline. Similar to the SAFE (albumin) trial, clinicians were permitted to resuscitate patients according to their own goals and preferences.
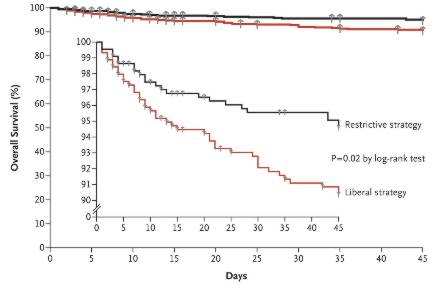
The primary outcome was death within 90 days. Secondary outcomes included acute kidney injury and failure and treatment with renal-replacement therapy.
There was no mortality difference. A total of 597 of 3315 patients (18.0%) in the HES group and 566 of 3336 (17.0%) in the saline group died (relative risk in the HES group, 1.06; 95% confidence interval [CI], 0.96 to 1.18; P=0.26). There was no significant difference in mortality in six predefined subgroups. Renal-replacement therapy was used in 235 of 3352 patients (7.0%) in the HES group and 196 of 3375 (5.8%) in the saline group (relative risk, 1.21; 95% CI, 1.00 to 1.45; P=0.04).
HES was associated with less renal injury than saline, by RIFLE criteria, but post hoc creatinine and urinary output were worse for HES In the HES and saline groups, renal injury occurred in 34.6% and 38.0% of patients, respectively (P=0.005), and renal failure occurred in 10.4% and 9.2% of patients, respectively (P=0.12). There was a 1.2% absolute increase in the risk of needing renal replacement therapy (p<;0.5) in the HE’S group.
HES was associated with significantly more adverse events (5.3% vs. 2.8%, P<;0.001). These included itching, skin rash and “other” (not explained).
A few comments: the mortality rate for a critical care study was astonishingly low, suggesting that the addition of surgical patients (42%) and some entry restrictions may have biased the study [Of the 7000 patients 2,876 were admitted from the operating room]. Almost 10% of patients came from another hospital. Only 1 in 4 came from the emergency department. So there is likely lead-time bias (incidentally, this distribution is near identical to the 6S study. It is highly unlikely that the majority of patients received, exclusively, one of these investigation fluids prior to ICU admission. Patients were in the ICU for 10 or 11 hours prior to randomization: the “golden window”. The patients should have been resuscitated by this stage. This is suggested by the almost ludicrously small amount of fluid that patients received day 0 (see below).
As expected HES patients received less fluid early on, but this did not translate into better outcomes. What is surprising is how little fluid the patients received in the first 24 hours (1500ml to <;2000ml net fluid balance). Patients received between 1000ml (HES) and 1500ml (IS) in addition to study fluids. In fact they seem to have gotten a lot more non study fluid than study fluid. This is presumably due to the 50ml/kg limit (400ml for an 80kg patient). As the on study fluid of choice was IS, this was really a crystalloid plus colloid versus crystalloid study. Indeed patients almost exclusively received IS
It is remarkable how little fluid the patients accumulated over the first 3 days (by the end of day 3 the IS group appear to have a net negative balance). What ever way you look at it, patients received significantly less fluid than in the 6S study (nearly 6L day 1). I return to my previous observations: nearly 50% surgical patients, with resolving stress responses, patients probably already resuscitated before randomized to the study.
It would have useful to know the electrolyte and acid base status. These patients all received a lot of chloride: what proportion of the had hyperchloremic acidosis?
It is very hard to make anything of the renal function tests in this study. On first sight the 36% rate of renal dysfunction at baseline was similar to 6S. But Scandanavian patients were significantly sicker. They had a mortality rate of 43-50%, consistent with other sepsis trials (such as VISEP). RRT use in the 6S study was 16% in the Ringer’s acetate group versus 5.8% in the IS group in this study. So I would be inclined to ignore RIFLE numbers and consider “real” kidney injury to be represented by the need for RRT.
So, how to evaluate this study? Does this study demonstrate the safety of HES in critical illness? No, it just shows that HES doesn’t increase mortality versus isotonic saline. They may be equally bad. Does this paper conflict with the 6S study? Only 30% of patients in the study were septic, the mortality was substantially lower in this study and it is likely that HES worsens outcomes in patients that require more of it (i.e. sicker patients). The onus of proof is on the intervention: HES demonstrates no mortality advantage over crystalloid, it may worsen outcome, it may be associated with more organ (particularly kidney) dysfunction. I am less likely to use these products in ICU. However, there is still a small argument for colloid administration in the peri operative period based on a series of oesophageal Doppler studies (from the UK). It is highly unlikely that 500ml HE’S will harm a patient. However, I don’t quite see the point: HES is expensive compared with crystalloid and only appears to have a marginally better volume expanding effect: why take the risk without clear benefit.
I presume some clever scientist will take this, the 6S and other crystalloid-colloid studies and inform us about all of the residual questions in a nice meta-analysis. In the near future, it would be helpful if the CHEST investigators would give us data on chloride levels and acid-base status. Perhaps their next study should be to compare isotonic saline to balanced salt solutions.
Finally, congrats again to the ANZICS trial group for showing the rest of us what can be done.

 The SOLAR trial, which compared a composite outcomes in perioperative colorectal or orthopaedic patients, assigned to Lactated Ringers’ (similar to Hartmann’s) solution – over 2 week blocks over a few years (8,616), has been published this month in Anesthesiology. The median volume of fluid administered in the perioperative period was 1.9L, and, no surprise here – there was no difference in outcomes.
The SOLAR trial, which compared a composite outcomes in perioperative colorectal or orthopaedic patients, assigned to Lactated Ringers’ (similar to Hartmann’s) solution – over 2 week blocks over a few years (8,616), has been published this month in Anesthesiology. The median volume of fluid administered in the perioperative period was 1.9L, and, no surprise here – there was no difference in outcomes.