The 2025 Western Anaesthesia Symposium, our 44th, is in the Salthill Hotel, on the Promenade in Galway on April 4th and 5th 2025.

Tickets are available here
Download the Abstract Submission Form below:

The 2025 Western Anaesthesia Symposium, our 44th, is in the Salthill Hotel, on the Promenade in Galway on April 4th and 5th 2025.
Tickets are available here
Download the Abstract Submission Form below:
 Twenty years ago perioperative myocardial ischaemia was a relatively easy thing to diagnose – we checked ECG looking for ST segment and T wave changes, and looked for an MB-CK rise. Then troponin arrived, and suddenly the proportion of patients with perioperative ischaemia increased drastically. For many of us, the report of a “postoperative troponin leak” results in a shoulder shrug: we don’t know what it means, we don’t really know the long term implications.
Twenty years ago perioperative myocardial ischaemia was a relatively easy thing to diagnose – we checked ECG looking for ST segment and T wave changes, and looked for an MB-CK rise. Then troponin arrived, and suddenly the proportion of patients with perioperative ischaemia increased drastically. For many of us, the report of a “postoperative troponin leak” results in a shoulder shrug: we don’t know what it means, we don’t really know the long term implications.
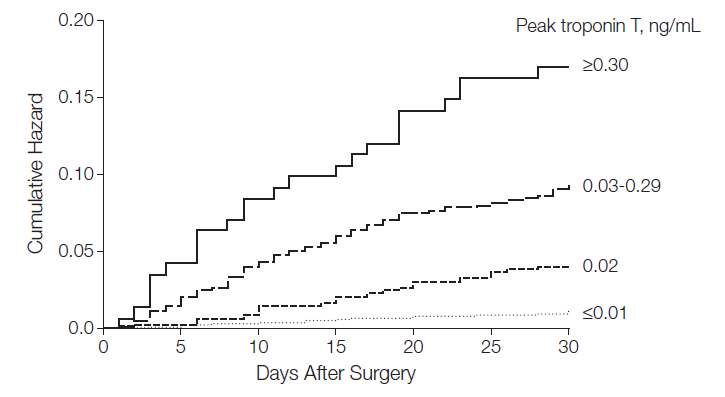
Thankfully, a landmark study, VISION (click here), has provided us with quality epidemiologic data. This was a cohort study of 15000 patients >45 years that underwent non cardiac surgery and had troponin T (TnT) measured in the first 3 postoperative days. All patients had to have procedures that required overnight stay in hospital. The main outcome measure was 30 day mortality.
After 30 days 1.9% of patients had died. Patients were more likely to die if their peak TnT level was 0.02 ng/ml (versus reference range of <0.01 ng/ml). This occurred in 11.6% of patients. The greater the TnT level, the more likely the patient was to die. They were able to stratify risk depending on TnT levels. Patients with a peak TnT value of 0.01 ng/mL or less, 0.02, 0.03-0.29, and 0.30 or greater had 30-day mortality rates of 1.0%, 4.0%, 9.3%, and 16.9%, respectively (figure above).
Risk was expressed in terms of Hazard Ratio (HR): greater HR = more likely adverse outcome with 1 being equivalent to no additional risk, <1 lower risk, >1 higher risk. Peak TnT of 0.02 ng/mL (adjusted hazard ratio [aHR], 2.41; 95% CI, 1.33-3.77); 0.03 to 0.29 ng/mL (aHR, 5.00; 95% CI, 3.72-6.76); and 0.30 ng/mL or greater (aHR, 10.48; 95% CI, 6.25-16.62).
Who was at increased risk? The older the patient the higher the risk. Emergency surgery, general surgery, neurosurgery were associated with increased risk. Vascular surgery was not, although the presence of peripheral vascular disease, COPD, previous stroke, coronary arterial disease and cancer did predict adverse outcome. Diabetes, obesity, afib, OSA, hypertension, orthopaedic/thoracic urology surgery – did not predict adverse events.
Conclusions: these data demonstrate the efficacy of TnT measurement in determining perioperative prognosis. 1in 25 patients with a peak TnT measurement of 0.02ng/mL,1 in11patients with a peak TnT measurement of 0.03 to 0.29ng/mL, and 1 in 6 patients with a peak TnT measurement of at least 0.30ng/mL will die within 30 days of surgery. Two questions arise from this study: 1. should we be routinely measuring TnT postoperatively in surgical inpatients >45 years; 2. If the patient has a troponin leak – what should be do then: PCI, aspirin, clopidogrel, statins, betablockers, all of the above, none of them? Will routine measurement of TnT result in a dramatic increase in cardiology consultations with little evidence that there are interventions that may improve outcomes in this setting?
Anecdotally, the majority of anesthetists withhold ACE inhibitors (angiotensin converting enzyme inhibitors ACEI) on the day of surgery because of concerns regarding hypotension, particularly in operations that may involve sympathectomy (spinal anesthesia) or blood loss. This appears to be a particular problem with angiotensin receptor blockers (here). We already know that withholding beta blockers and statins preoperatively is associated with an increase in the risk of myocardial ischaemia (reviewed here). ACEI were the wonder drugs of the 1980s: 1. use of ACE inhibitors provide long-term cardiovascular protection and reduce ischemic events and complications; 2. early ACE inhibitor therapy has been demonstrated to produce improved survival and heart function benefits in patients with acute myocardial infarction; 3. they are remarkably effective drugs in the treatment of heart failure and hypertension; 4. ACEI delays the progression of diabetic nephropathy. So, is it wise to withhold these drugs in the preoperative period?
The following is a quote from a review on this topic in the Postgraduate Medical Journal: “The use of these agents before surgery has been associated with a variable incidence of hypotension during the initial 30 min after induction of anaesthesia; however, these hypotensive episodes have not been conclusively linked to any significant postoperative complications…” (here).
The following is a quote from an excellent review of the topic of drug withholding in preoperative patients: ACEI “intensify the hypotensive effects of anesthesia induction. Because angiotensin II plays a key role in maintaining circulating volume in response to stressors, volume deficits can occur in ACE inhibitor-treated patients as angiotensin II cannot compensate for venous pooling of blood, resulting in diminished cardiac output and arterial hypotension. However, continued renin-angiotensin system suppression may protect regional circulation, as has been demonstrated by reduced release of cardiac enzymes with ACE inhibitor continuation (compared with interruption) in cardiac surgery patients. ACE inhibitors also have a renal protective effect, preserving glomerular filtration rate in patients undergoing aortic abdominal aneurysm repair or coronary artery bypass graft surgery. Hypotension with ACE inhibition is treatable with sympathomimetics, alpha-agonists, and intravenous fluids.” (here). Essentially the author is referring to phenylephrine and vasopressin.
So, it may surprise you to discover that there are emerging data to support the continuation of ACEI in the preoperative setting, particularly in cardiac surgery patients. A recent article in circulation (here – subscription required – the HSE has a 1 year embargo – cheapskates!) suggests that withholding ACEI after cardiac surgery is associated with increased incidence of non fatal cardiac events:
This was a “prospective observational study of 4224 patients undergoing coronary artery bypass graft surgery (CABG). The cohort included 1838 patients receiving ACEI therapy before surgery and 2386 (56.5%) without ACEI exposure. Postoperatively, the pattern of ACEI use yielded 4 groups: continuation, 915 (21.7%); withdrawal, 923 (21.8%); addition, 343 (8.1%); and no ACEI, 2043 (48.4%). Continuous treatment with ACEI versus no ACEI was associated with substantive reductions of risk of nonfatal events (adjusted odds ratio for the composite outcome, 0.69; 95% confidence interval, 0.52–0.91;P=0.009) and a cardiovascular event (odds ratio, 0.64; 95% confidence interval, 0.46–0.88; P=0.006). Addition of ACEI de novo postoperatively compared with no ACEI therapy was also associated with a significant reduction of risk of composite outcome (odds ratio, 0.56; 95% confidence interval, 0.38–0.84; P=0.004) and a cardiovascular event (odds ratio, 0.63; 95% confidence interval, 0.40–0.97;P=0.04). On the other hand, continuous treatment of ACEI versus withdrawal of ACEI was associated with decreased risk of the composite outcome (odds ratio, 0.50; 95% confidence interval, 0.38–0.66; P<0.001), as well as a decrease in cardiac and renal events (P<0.001 and P=0.005, respectively).”
There are some unpublished data that continuing ACCEI up to surgery (and presumably afterwards) is associated with lower 30 day mortality (here). Preoperative use appears to be associated with fewer major adverse events after cardiac surgery (here), and even when no benefit has been demonstrated the agents appear to be safe (here).
So, think twice before you stop the ACEI in your preoperative visit. Nevertheless, I am still going to avoid these agents when anesthetizing patients in the beach chair position (here).
 Alas – another intervention bites the dust. For decades the intra-aortic balloon pump has been heralded as the great savior of the patient with cardiogenic shock. If you have always found these devices confusing (when to use, when to wean, what difference 1:1 versus 1:2 augmentation etc), then worry not: they are heading to the Swan Ganz junkyard. In this week’s NEJM the IABP-SHOCK II trial is published (read here). Six hundred patients were recruited in 37 locations in Germany in 3 years – randomized to IAB-counterpulsation at 1:1 or control, essentially catecholamine, therapy. Patients were eligible for the trial if they had had any form of myocardial infarction complicated by cardiogenic shock, or needed an emergency percutaneous coronary intervention. The majority of patients had PCIs and the IABP could be placed before or after.
Alas – another intervention bites the dust. For decades the intra-aortic balloon pump has been heralded as the great savior of the patient with cardiogenic shock. If you have always found these devices confusing (when to use, when to wean, what difference 1:1 versus 1:2 augmentation etc), then worry not: they are heading to the Swan Ganz junkyard. In this week’s NEJM the IABP-SHOCK II trial is published (read here). Six hundred patients were recruited in 37 locations in Germany in 3 years – randomized to IAB-counterpulsation at 1:1 or control, essentially catecholamine, therapy. Patients were eligible for the trial if they had had any form of myocardial infarction complicated by cardiogenic shock, or needed an emergency percutaneous coronary intervention. The majority of patients had PCIs and the IABP could be placed before or after.
There is a widespread belief that using IABP improves pump function, restoring cardiovascular health and preventing the development of multi-organ failure. The primary endpoint of the study was 30 day all cause mortality. This is a flawed measure in critical care, as many patients will still be alive at 30 days, awaiting withdrawal of life sustaining therapy. The authors are in the process of collecting 90 day and 6 month data. The authors also looked for evidence of multi-organ failure (using SAPS II), infectious and ischaemic (using lactate) complications.
Previous studies have reported mortality rates of 42-48% in cardiogenic shock. The authors reported 30 day mortality of 39.7% in the IABP group and 41.3% in the control group (not significant). There was no significant difference in any of the other endpoints either..
Criticisms and generalizability? The mortality rate was lower than expected, but this was a heterogenous German population, a single health system, with an average BMI of 27. So maybe the patients were less unhealthy than comparable North American Studies. More likely, the IABP can be added to a long list of devices that receive religious like devotion, but have little clinical benefit. Further data of interest would be whether or not IABP really benefits postoperative cardiac patients. In the meantime, it is likely that we will encounter these devices less frequently in the future.
