
 A half generation ago, the TRICC trial (here) suggested that routine blood transfusion in critically ill patients did not confer benefit if the haemoglobin level was above 7g/dl. This resulted in a evidence based paradigm for lower transfusion triggers. The problem was – how do you deal with the bleeding patients?
A half generation ago, the TRICC trial (here) suggested that routine blood transfusion in critically ill patients did not confer benefit if the haemoglobin level was above 7g/dl. This resulted in a evidence based paradigm for lower transfusion triggers. The problem was – how do you deal with the bleeding patients?
A recent study in NEJM (here) looked at liberal versus restrictive transfusion practices on patients admitted with gastrointestinal bleeding.
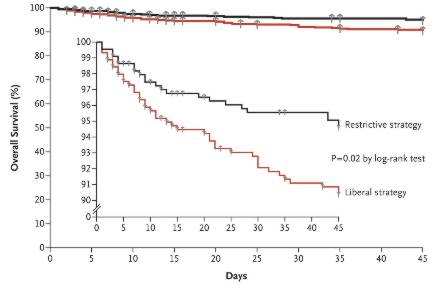
921 patients with severe acute upper gastrointestinal bleeding were included in the study: and 461 of them were randomly assigned to a restrictive strategy (transfusion when the hemoglobin level fell below 7 g per deciliter) and 460 to a liberal strategy (transfusion when the hemoglobin fell below 9 g per deciliter). Randomisation was stratified according to the presence or absence of hepatic cirrhosis.
Substantially more patients in the liberal strategy group received transfusion: 395 (85%) versus 236 (49%) liberal versus restrictive (P<0.001). The conventional wisdom would hold that greater oxygen carrying capacity in the liberal group would result in better outcomes. The null hypothesis would be that there was no difference. However, the patients in the restrictive group had BETTER OUTCOMES. The hazard ratio for 6 week mortality was 0.55; 95% confidence interval [CI], 0.33 to 0.92; P=0.02) [with HR a number of <1 reflects benefit, >1 reflects injury]. The absolute risk reduction was 4% (5% restrictive, 9% liberal p = 0.02; NNT 25). In addition, patients in the liberal strategy group had a 6% absolute increase (number needed to injure 16; (P=0.01) ) in the risk of further bleeding.
There was an absolute risk reduction of adverse events of 8% in the restrictive group (NNT 12; p = 0.02). Restrictive transfusion also resulted in better survival in patients with peptic (gastric or duodenal) ulcers, and those with mild to moderate cirrhosis.
Why would bleeding patients do better if transfusions are witheld? There are many potential reasons: 1. The concept of damage control resuscitation: teleologically we have evolved to handle hypovolaemia and can survive considerable blood loss. Blood transfusion without source control may cause clots to destabilise and further bleeding to occur. 2. Blood is immunosuppressive: patients who are transfused are at elevated risk of infectious complications. 3. In this particular study patients in the liberal transfusion group had higher portal pressures and were more likely to rebleed (but so too were patients with peptic ulcers). 4. Transfusion may result in volume overload, abdominal compartment syndrome, myocardial ischaemia and transfusion related lung injury.
What are the implications of this study. Approach with caution! This study does not license clinicians to withhold blood from ex-sanguinating patients. Nor does it prove anything about transfusion in the setting of non gastrointestinal blood loss. However, it does provide us with further information about the safety and implications of blood transfusion in a specific setting. Allied with accumulating data detailing the hazards of colloid transfusion, adverse outcomes associated with crystalloid over-resuscitation, and the ongoing controversy regarding albumin – one has to wonder where we are with fluid resuscitation. Remembering that red cell transfusion is a key component of the Rivers’ surviving sepsis protocol, one wonders if this is the first real nail in the coffin for that approach.
Comments are welcome here.
