
 Twenty years ago perioperative myocardial ischaemia was a relatively easy thing to diagnose – we checked ECG looking for ST segment and T wave changes, and looked for an MB-CK rise. Then troponin arrived, and suddenly the proportion of patients with perioperative ischaemia increased drastically. For many of us, the report of a “postoperative troponin leak” results in a shoulder shrug: we don’t know what it means, we don’t really know the long term implications.
Twenty years ago perioperative myocardial ischaemia was a relatively easy thing to diagnose – we checked ECG looking for ST segment and T wave changes, and looked for an MB-CK rise. Then troponin arrived, and suddenly the proportion of patients with perioperative ischaemia increased drastically. For many of us, the report of a “postoperative troponin leak” results in a shoulder shrug: we don’t know what it means, we don’t really know the long term implications.
Thankfully, a landmark study, VISION (click here), has provided us with quality epidemiologic data. This was a cohort study of 15000 patients >45 years that underwent non cardiac surgery and had troponin T (TnT) measured in the first 3 postoperative days. All patients had to have procedures that required overnight stay in hospital. The main outcome measure was 30 day mortality.
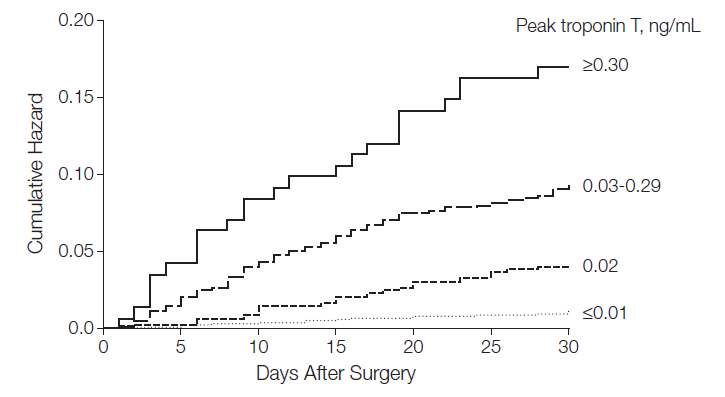
After 30 days 1.9% of patients had died. Patients were more likely to die if their peak TnT level was 0.02 ng/ml (versus reference range of <0.01 ng/ml). This occurred in 11.6% of patients. The greater the TnT level, the more likely the patient was to die. They were able to stratify risk depending on TnT levels. Patients with a peak TnT value of 0.01 ng/mL or less, 0.02, 0.03-0.29, and 0.30 or greater had 30-day mortality rates of 1.0%, 4.0%, 9.3%, and 16.9%, respectively (figure above).
Risk was expressed in terms of Hazard Ratio (HR): greater HR = more likely adverse outcome with 1 being equivalent to no additional risk, <1 lower risk, >1 higher risk. Peak TnT of 0.02 ng/mL (adjusted hazard ratio [aHR], 2.41; 95% CI, 1.33-3.77); 0.03 to 0.29 ng/mL (aHR, 5.00; 95% CI, 3.72-6.76); and 0.30 ng/mL or greater (aHR, 10.48; 95% CI, 6.25-16.62).
Who was at increased risk? The older the patient the higher the risk. Emergency surgery, general surgery, neurosurgery were associated with increased risk. Vascular surgery was not, although the presence of peripheral vascular disease, COPD, previous stroke, coronary arterial disease and cancer did predict adverse outcome. Diabetes, obesity, afib, OSA, hypertension, orthopaedic/thoracic urology surgery – did not predict adverse events.
Conclusions: these data demonstrate the efficacy of TnT measurement in determining perioperative prognosis. 1in 25 patients with a peak TnT measurement of 0.02ng/mL,1 in11patients with a peak TnT measurement of 0.03 to 0.29ng/mL, and 1 in 6 patients with a peak TnT measurement of at least 0.30ng/mL will die within 30 days of surgery. Two questions arise from this study: 1. should we be routinely measuring TnT postoperatively in surgical inpatients >45 years; 2. If the patient has a troponin leak – what should be do then: PCI, aspirin, clopidogrel, statins, betablockers, all of the above, none of them? Will routine measurement of TnT result in a dramatic increase in cardiology consultations with little evidence that there are interventions that may improve outcomes in this setting?

Its interesting that vascular surgery was not associated with increased risk Pat. ACC/AHA guidelines put vascular surgery patients in their own special risk box with specific guidelines in how we manage them preoperatively.
Also, its important that we recognise the specific risk that applies to the general surgical patient. Colorectal surgery carries with it a significant 30 day mortality of 6.7% in the UK. Compare that to around 2% for cardiac surgery!